



Learn more about the role of the urologist and the importance for a patient to gather adequate information after receiving a prostate cancer diagnosis.
A man with prostate cancer shares the challenges of his cancer experience.
You’ve been diagnosed with prostate cancer? Your role is as important as that of your medical team.

Recently diagnosed with cancer? Educate yourself to fully understand your situation.
After a prostate cancer diagnosis, questions about survival, cure rates, and quality of life can arise.

This webinar covers various tests and exams for diagnosing and monitoring prostate cancer.
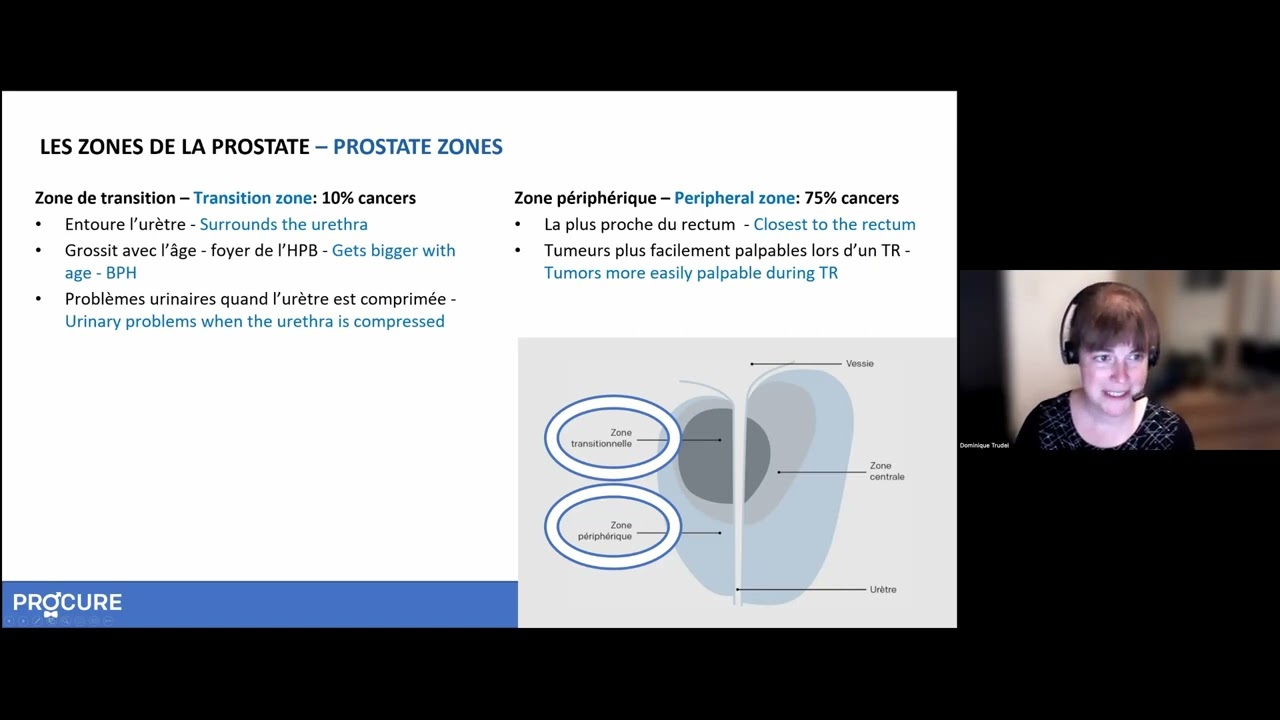
This webinar clarifies biopsy reports, pathologists’ roles, and how results confirm or rule out prostate cancer.

After receiving a diagnosis of prostate cancer, you will undoubtedly have questions about your prognosis and survival and will want to know the chances of success with your treatment.

Do you have a significant family history of cancer? Is there a link between prostate cancer and a genetic mutation?

Prostate cancer often overwhelms patients. Finding the right words is crucial to comfort and support them.

If you are obese or overweight, it is more likely that prostate cancer will be diagnosed at a more advanced stage…

It depends on the definition of old. Is being 50 years old really considered “old”?

As a woman, you might think that prostate cancer is not your concern because you don’t have a prostate. However, prostate cancer is the most common cancer in men.

The PSA test should generally be offered to any man aged 50 and over with a life expectancy of at least ten years. So why this refusal?

Did you know that participating in a clinical trial advances medical science and improves the lot of patients for future generations?

Have you been diagnosed with prostate cancer? Your role as a patient is essential throughout your journey.